
-Acromegaly/Gigantism-
-Acromegaly is caused from excessive secretion of growth hormone (GH)
-most common cause of acromegaly is a somatotroph (GH) adenoma
-this causes fusion of the epiphyseal growth plates n a child or adolescent called pituitary gigantism
-metabolic effects include nitrogen retention, insulin antagonism, and lipolysis
-may get headache and/or vision loss
-if the macroademona is large, may get decreased secretion of other pituitary hormones
-may get skin overgrowth and skin thickening
-may get macroglossia
-many organs can become enlarged including thyroid, heart, liver, lungs, and kidneys. Prostate enlargement may occur
-patients may get HTN, left ventricular hypertrophy, and cardiomyopathy
-patients with acromegaly have an increased risk of colon cancer
-Patients that have a resectable microadenoma or macroadenoma, these should be resected
-Somatostatin analogue treatment is an option
-If adenoma increases in size radiotherapy or repeat surgery is indicated
-Diabetes Insipidus-

-polyuria is urinary output greater than 3 liters per day
-Types of Diabetes Insipidus: Central diabetes insipidus, nephrogenic diabetes insipidus
-Can also have primary polydipsia where it is characterized by increased water intake, usually seen in those with psychiatric illness. Can be seen ion those taking phenothiazine therapy which has a side effect of dry mouth
-Central Diabetes Insipidus-is characterized by deficient secretion of antidiuretic hormone (ADH). Common causes include trauma, pituitary surgery, and hypoxic or ischemic encephalopathy
-Nephrogenic Diabetes Insipidus-has normal ADH but the kidney has varying degrees of resistance to its renal retaining effects. If seen during childhood is due to inherited defects. Adults is usually acquired and secondary to lithium use and hypercalcemia
-low plasma sodium concentration an low urine osmolality is due to overload from primary polydipsia
-a high to normal plasma sodium concentration and low urine osmolality is less than plasma, points to diagnosis of diabetes insipidus
-a normal plasma sodium concentration with a urine osmolality more than 600 excludes the diagnosis of diabetes insipidus
-water restriction test is raising the plasma osmolality by either water restriction or administration of hypertonic saline (0.05 mL/kg/min) for no more than 2 hours.
-raising plasma osmolality leads to progressive ADH release and increase in urine osmolality in normal patients
-once the plasma osmolality reaches 295-300 or the plasma sodium is 145 or higher, the effect of endogenous ADH is maximal. Administering ADH at this point will not elevate urine osmolality unless ADH release is impaired (except patients with central diabetes insipidus)
-the water restriction tests involves measurement of the urine volume and osmolality every hour and the plasma sodium concentration and osmolality every 2 hours. The patient should not drink 2-3 hours before the test
-End point for the water restriction test is when the urine osmolality reaches normal value above 600 (means normal ADH release)
-also when the urine osmolality is stable on 2 or 3 consecutive measurements, with a rising plasma osmolality
-also when the plasma osmolality exceeds 295-300 or the plasma sodium is over 145.
-desmopressin is administered
-plasma and urine ADH levels should be measured if the response to the water restriction test is equivocal
-Central DI-ADH release and urine and plasma osmolality may rise submaximally. Desmopressin will rise urine osmolality
-Nephrogenic DI-has a submaximal rise in urine osmolality in response to water restriction. The plasma osmolality stimulates ADH release. This will produce a modest increase in urine osmolality due to resistance to ADH
-Patients with Central DI or Nephrogenic DI present with polyuria, polydipsia, and nocturia
-Treatment of Central Diabetes Insipidus involves Desmopressin which is the preferred medication
-A low solute and sodium diet should be instituted
-Desmopressin has little effect on nephrogenic diabetes insipidus
-Dwarfism-

-Dwarfism is defined as usually a height less than 4 feet 10 inches
-It is caused by multiple medical condition
-Achondroplasia accounts for 70-80 percent of the cases
-Turner syndrome and growth hormone deficiency can be traced to some of the cases of dwarfism
-Three to thirty percent of children with growth hormone deficiency have a parent, sibling or child affected
-Short stature is a term applied to child who is two standard deviation below the mean
-Idiopathic short stature is when there is no endocrine, metabolic, or other diagnostic cause
-Intrinsic short stature is a normal family variant
-Delayed growth and puberty usually is due to under nutrition
-Attenuated growth usually results from metabolic or endocrine disorders or severe systemic illness
-Endocrine causes include Vitamin D deficiency or resistance, growth hormone deficiency, growth hormone insensitivity, and hypothyroidism
-Glucocorticoid therapy long term effects endogenous growth hormone secretion
-Autoimmune Diabetes Mellitus can cause attenuated growth
-Growth hormone deficiency results from deficiency of the growth hormone releasing hormone (GHRH) but can be because of sellar and presellar tumors
-Treatment is targeted at finding the cause and reversing what can be reversed
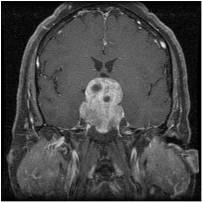
-Neoplastic Disease-
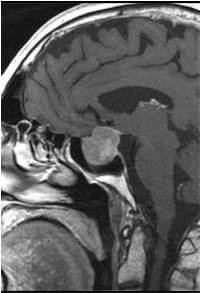
-There are other sellar lesions that are not adenomas, but cannot be differentiated from other adenomas until biopsy.
-Craniopharyngiomas are mixed solid and cystic lesions that arise from remnants of Rathke's pouch. It is a benign lesion
-Meningioma-usually benign lesion that comes from the meninges and can be anywhere in the head
-Pituicytoma-uncomon glioma that arises from the posterior pituitary. Has no known hormonal function.
-Germ Cell Pituitary Tumors-they are also ectopic pinealomas that are malignant and present with headache, nausea, vomiting, and lethargy, diplopia, and can have diabetes insipidus. These usually respond well to radiation. Human Beta HCG and alpha fetal protein can be increased.
-Chordomas-locally aggressive tumors that metastasize from the Pituitary gland. They present with headaches, vision disturbances, and anterior pituitary hormone abnormalities. It is a malignant tumor
-Primary Central Nervous System Lymphoma-sometimes involves both the pituitary any hypothalamus. It is a malignant tumor
-One to two percent of sellar masses involve metastasis from a distant site. Most commonly it occurs with breast cancer in women and lung cancer in men.
-Adenomas-
-Lactotroph Pituitary Adenoma- dopamine agonist should be used for decreasing adenoma size. These can be very large and cause visual defects
-Somatotroph Pituitary Adenomas-cause acromegaly. They are confined to the sella. If these tumors impair vision, surgical removal is recommended. Surgery offers a rapid cure of acromegaly.
-Corticotroph Pituitary Adenomas-no matter if they are micro or macro adenomas surgery is recommended first line. Before surgery you want to confirm Cushing Syndrome and demonstrate the adenoma is the source of the excessive ACTH secretion
Hello viewer’s
ReplyDeleteI don’t have much to say there are so may scammers going on online so we cant detect the real herbal medicine doctors. Thank GOD for leading me, please don’t ignore this post is real Dr Emmanuel, is a real herbal Doctor, he cured me from Brain tumor, i am living so happy and free , i was fully recovered within 4 weeks of usage of dr Emmanuel herbal medicine ,please viewers out there that have any deadly disease don't fail to contact him via his email; nativehealthclinic@gmail.com or WhatsApp/Call: +2348140073965 thanks once again to dr Emmanuel GOD bless you abundantly
Hello viewer’s
ReplyDeleteI don’t have much to say there are so may scammers going on online so we cant detect the real herbal medicine doctors. Thank GOD for leading me, please don’t ignore this post is real Dr Emmanuel, is a real herbal Doctor, he cured me from Brain tumor, i am living so happy and free , i was fully recovered within 4 weeks of usage of dr Emmanuel herbal medicine ,please viewers out there that have any deadly disease don't fail to contact him via his email; nativehealthclinic@gmail.com or WhatsApp/Call: +2348140073965 thanks once again to dr Emmanuel GOD bless you abundantly